Delirium VULnerability in GEriatrics (DIVULGE) 2 Study
Post-operative delirium is a common, distressing, and debilitating condition associated with significant long-term decline in older adults. The impact of delirium is enormous: it affects 25-40% of older-surgical patients and costs over $8.8 billion annually in Australia. We do not have good ways to stratify delirium risk pre-operatively, which would enable prevention efforts to be incorporated in perioperative care as well as shared decision making for older patients prior to surgery. This knowledge is especially important in the context of delirium subtypes (hypoactive, hyperactive and mixed), which demand different care and have different prognoses.
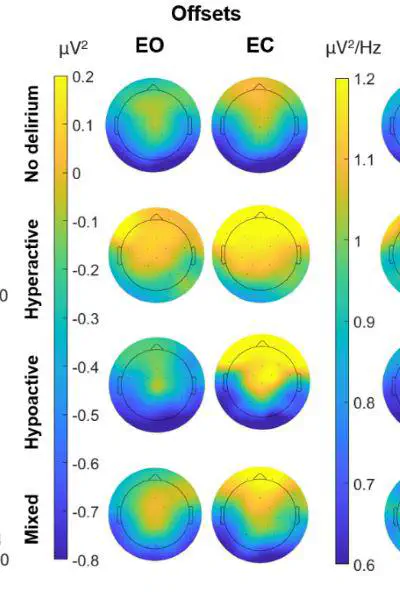
The underlying functional brain mechanisms of delirium vulnerability (risk for incident delirium) are yet to be determined. We have demonstrated that those at high risk for delirium subtypes show a specific pattern of neuropsychological performance and clinical characteristics. We also know that delirium is associated with a slowing of brain activity and reduced functional connectivity across a network of brain areas. Therefore, it is likely that patterns of brain activity will differ in those predisposed to developing delirium after a surgery, and that patterns are dependent on the subtype of delirium; our pilot data supports this proposition (Boord et al., 2014, Brain Communications).
Funded by a NHMRC Ideas grant, we will address this major gap by collecting brain activity data (electroencephalogram/EEG) from older adults before they undergo elective surgery (CALHN, NALHN and SAHLN). We will then measure delirium in hospital after surgery. By linking EEG data to delirium outcomes and using computational neuroscientific approaches which have never been used in the delirium field, we will determine brain activity patterns that discriminate between those who do and do not develop delirium after surgery, and further, how these patterns vary relative to subtype. With findings, we will co-design translational outcomes with patients and clinicians.
Key CAIN Lab members involved: Aaron Clark, Dr Daniel Feuerriegel (alumni) and Prof Hannah Keage
Professor Hannah Keage
Principal Investigator & Co-Director CAIN
I research the neurophysiology of cognitive ageing and delirium to develop evidence-based programs that support cognitive health in communities.